FUNGUS · Mold (monomorphic)
Aspergillus fumigatus
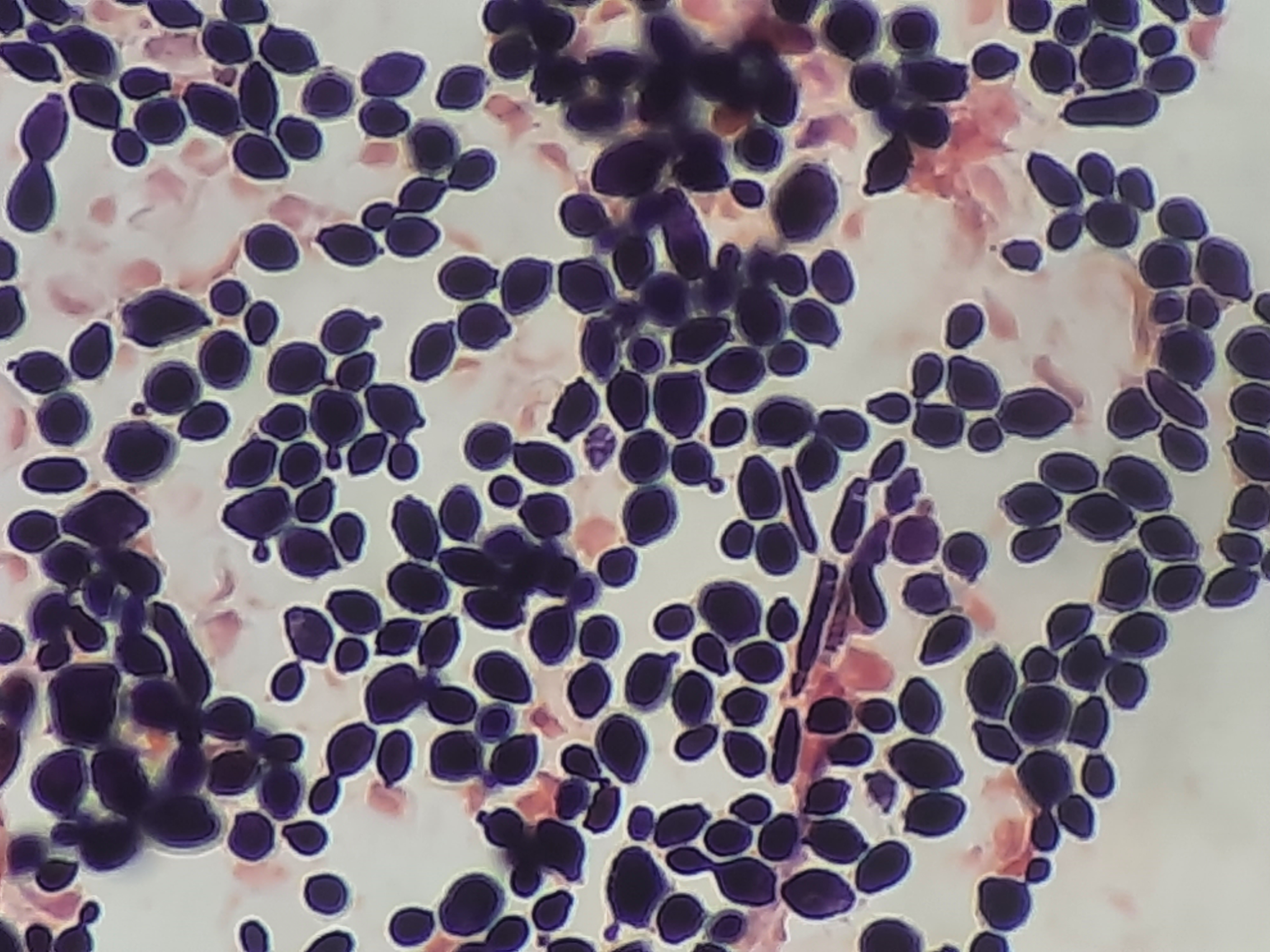
Aspergillus — Conidiophore microscopy (septate hyphae 45° branching)
Stain: Lactophenol cotton blue microscopy of conidiophoreMorphology: Septate hyphae branching at acute (~45°) angles, with conidiophores bearing radiating chains of conidia on a swollen vesicleYield: HIGHDifficulty: MEDIUM

Image: Wikimedia Commons · Ninjatacoshell (CC BY-SA 3.0)
Key facts
**Pathogenesis**: Ubiquitous airborne conidia; disease determined by host immune status — allergic (ABPA in asthma/CF), colonizing (aspergilloma in pre-existing cavity), or angioinvasive (neutropenic patients). **Diagnostic clue**: Septate hyphae with acute-angle branching on biopsy/silver stain (vs Mucor = nonseptate, 90° branching). Serum galactomannan and β-D-glucan; halo + air-crescent signs on chest CT. **Virulence**: Gliotoxin (immunosuppressive), elastase, vascular invasion.
Boards buzzwords
- septate hyphae
- 45° branching
- fungus ball / aspergilloma
- ABPA
- galactomannan
- halo and air-crescent signs
Associated diseases
- Allergic bronchopulmonary aspergillosis (ABPA) — asthma, CF
- Aspergilloma ('fungus ball' in old TB cavity)
- Invasive aspergillosis (neutropenic, transplant)
- Aspergillus sinusitis
Treatment
Voriconazole first-line for invasive aspergillosis; isavuconazole or liposomal amphotericin B alternatives; surgical resection for aspergilloma with massive hemoptysis; corticosteroids ± itraconazole for ABPA