BACTERIA · Spirochete
Treponema pallidum
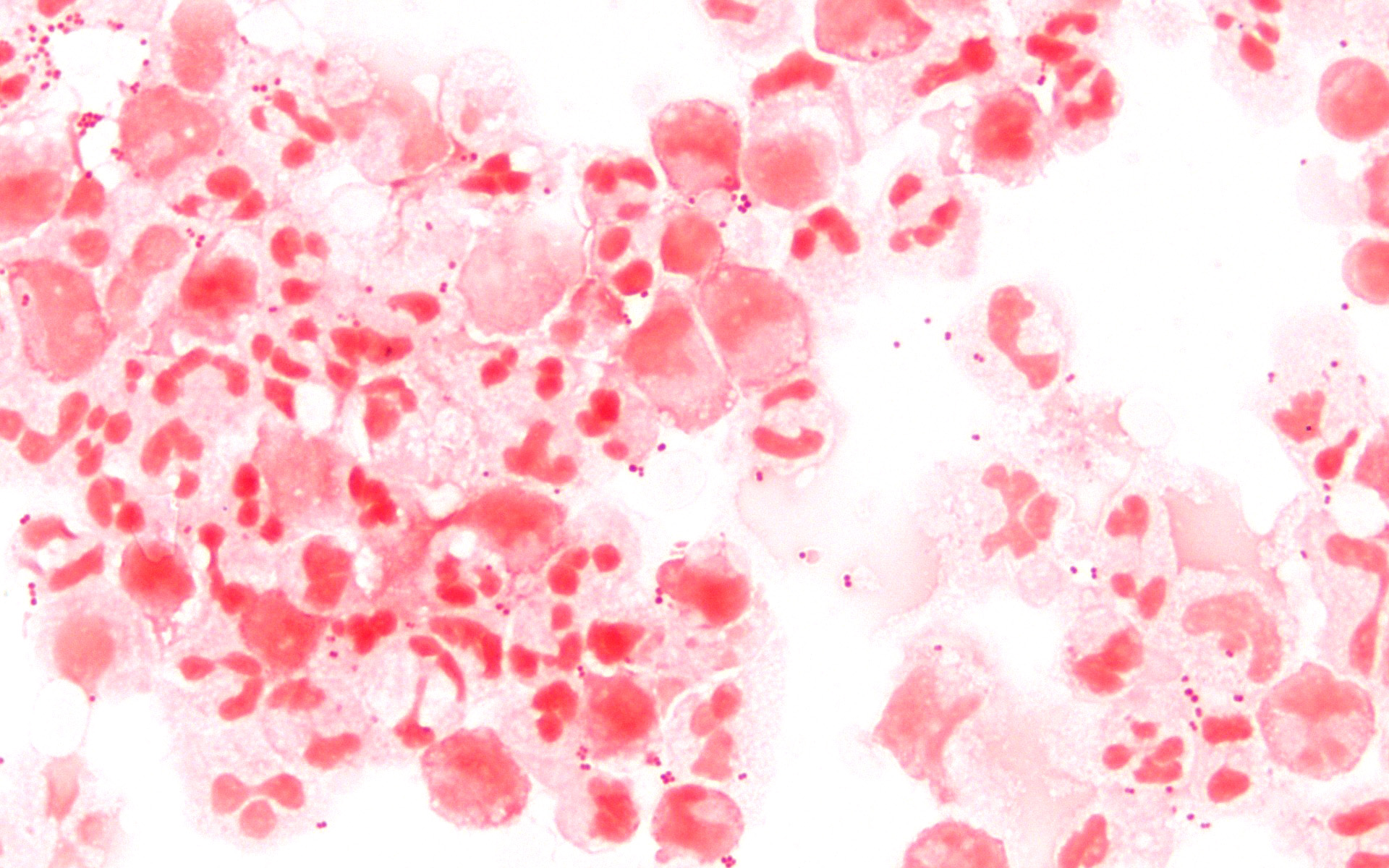
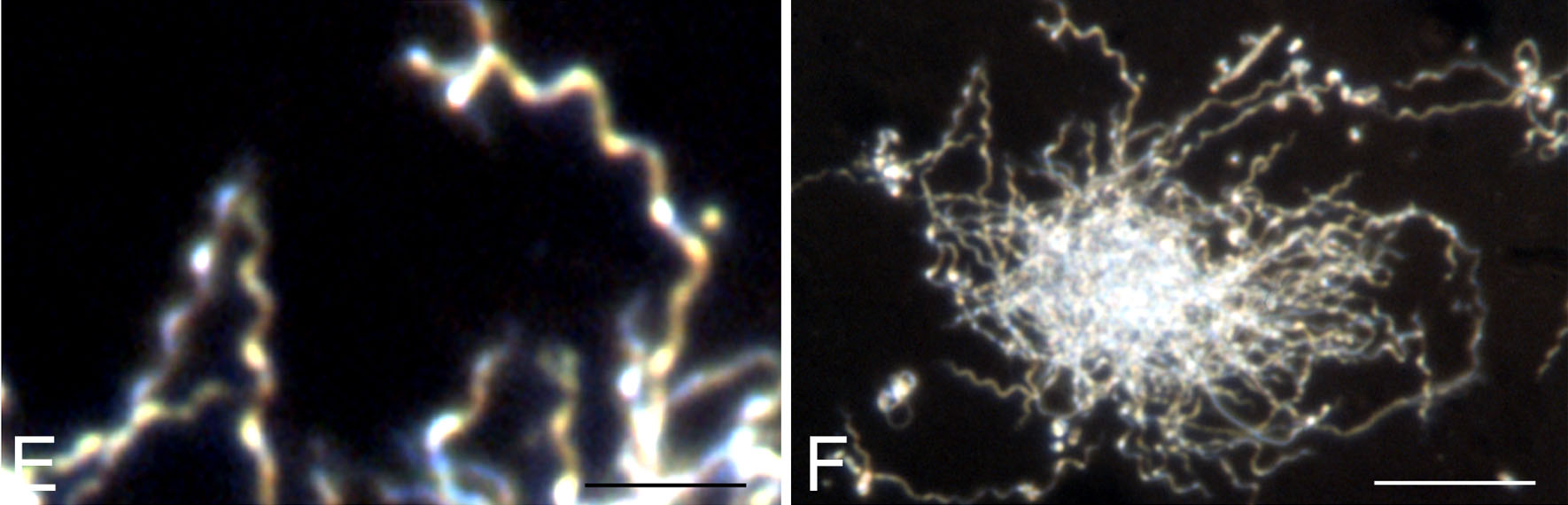
Treponema pallidum — Microscopy (syphilis spirochete)
Stain: Electron microscopy / dark-field equivalentMorphology: Long, slender, tightly coiled corkscrew-shaped spirocheteYield: HIGHDifficulty: MEDIUM
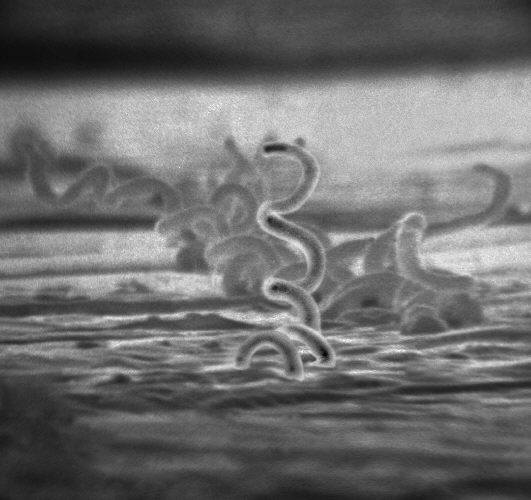
Image: Wikimedia Commons · File:Treponema_pallidum.jpg · CDC/PHIL (Public Domain)
Key facts
**Pathogenesis**: Cannot be Gram-stained or cultured — visualized only by dark-field microscopy or silver stain. Outer membrane is poorly antigenic → late disease driven by host immune response and obliterative endarteritis of vasa vasorum. **Diagnostic clue**: Dark-field of chancre exudate; nontreponemal screen (VDRL/RPR) confirmed with treponemal FTA-ABS or TP-PA. **Virulence**: Endoflagella for corkscrew motility, evasion via outer-membrane lipoproteins.
Boards buzzwords
- corkscrew motility
- painless chancre
- snail-track ulcers
- gummas
- tabes dorsalis
- Argyll Robertson pupil
- VDRL/RPR + FTA-ABS
Associated diseases
- Primary syphilis (painless chancre)
- Secondary (palms/soles rash, condyloma lata)
- Tertiary (gummas, aortitis, neurosyphilis — tabes dorsalis, paresis)
- Congenital syphilis
Treatment
Benzathine penicillin G IM — single dose for primary/secondary/early latent; 3 weekly doses for late latent; IV aqueous penicillin G × 10–14 days for neurosyphilis; doxycycline if non-pregnant penicillin allergic; watch for Jarisch-Herxheimer
Related organisms
Listeria monocytogenes
Gram-positive rod (facultative intracellular)

Mycobacterium tuberculosis
Acid-fast bacillus (mycolic acid cell wall)
Nocardia spp.
Gram-positive filamentous, partially acid-fast
Mycobacterium leprae
Acid-fast bacillus (obligate intracellular)
Neisseria meningitidis
Gram-negative diplococci
Borrelia burgdorferi
Spirochete